
Case Studies
-
A 65-year-old woman with a prior history of breast cancer and colon cancer is being followed with serum CEA measurements. The CEA has been steadily rising. An "incidental" 1.5 cm nodule of the right mid thyroid is palpated and FNA is performed.
Cytopathology
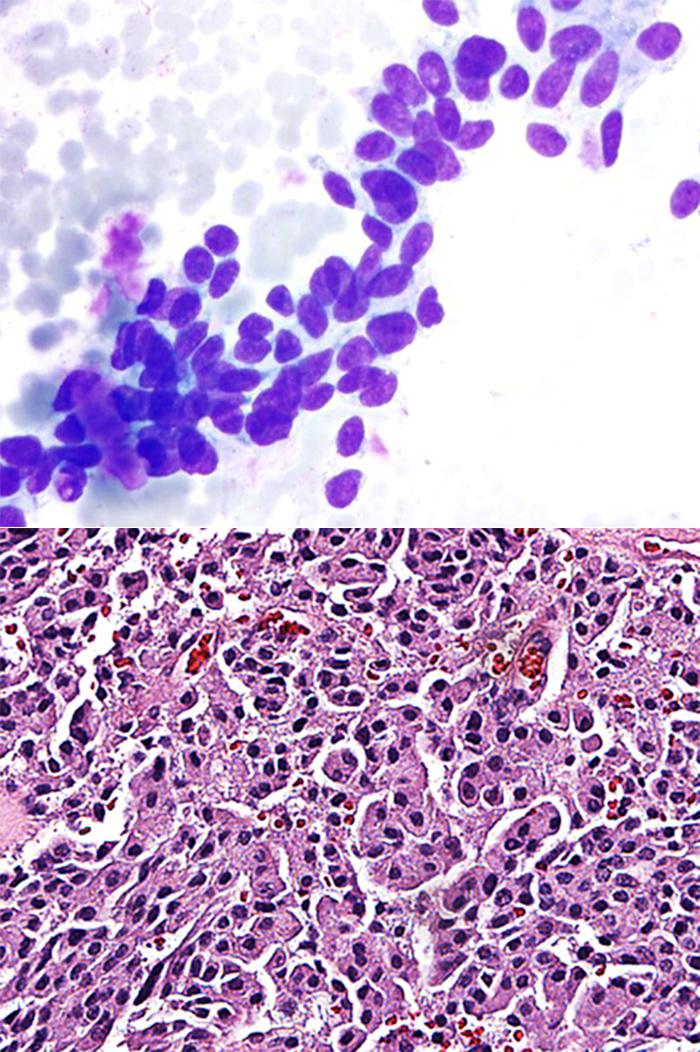
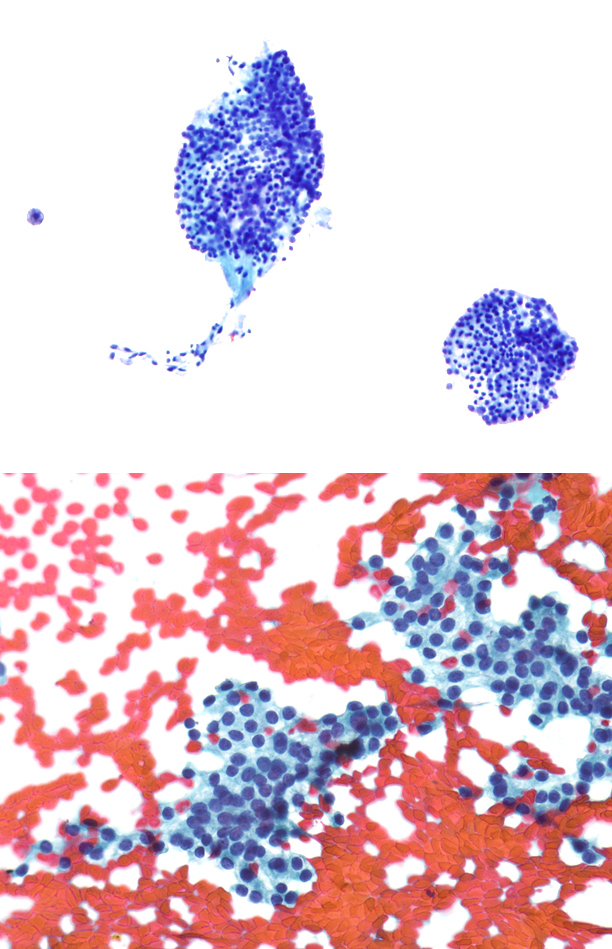
On the direct smears showed follicular cells, papillary structures, colloid and cyst contents were not present. At high magnification there was a non-cohesive small- or medium-sized neoplastic spindle cell population with a high nucleus-to-cytoplasmic (N:C) ratio. The nuclei were enlarged, oval to spindled and eccentrically-located. The nuclear chromatin pattern was variable, but appeared speckled “salt & pepper-like”. Nucleoli were not evident. A few cells with nuclear inclusions and grooves were identified (Fig. 1-1 TOP). There was inadequate material for ancillary immunohistochemical studies to confirm a diagnosis of medullary carcinoma. Thyroid mutation panel for ThyroSeq was performed.Diagnosis
Suspicious for Malignancy; Suspect Medullary Thyroid Carcinoma (Bethesda 2017 Category V). Thyroid mutation panel is requested.ThyroSeq Molecular Test Result.
Positive with expression of MTC gene.
Clinical management:
Follow-up serum calcitonin measurement was 1196. Pre-op evaluation did not indicate any syndrome, and family members had no related problems. Based on the pre-operative cytological diagnosis and ThyroSeq test result, a total thyroidectomy was performed. Histologic diagnosis was medullary thyroid carcinoma (Fig. 1-2BOTTOM). Ten years later, the patient is free of disease.
-
A 74-year-old woman who had a total thyroidectomy for malignancy about 20 years previously and a nephrectomy for renal cortical adenocarcinoma about 3 years previously presents with hypercalcemia. A 1cm. nodule is identified in the thyroid bed, and sono-guided FNA is performed.
Cytopathology
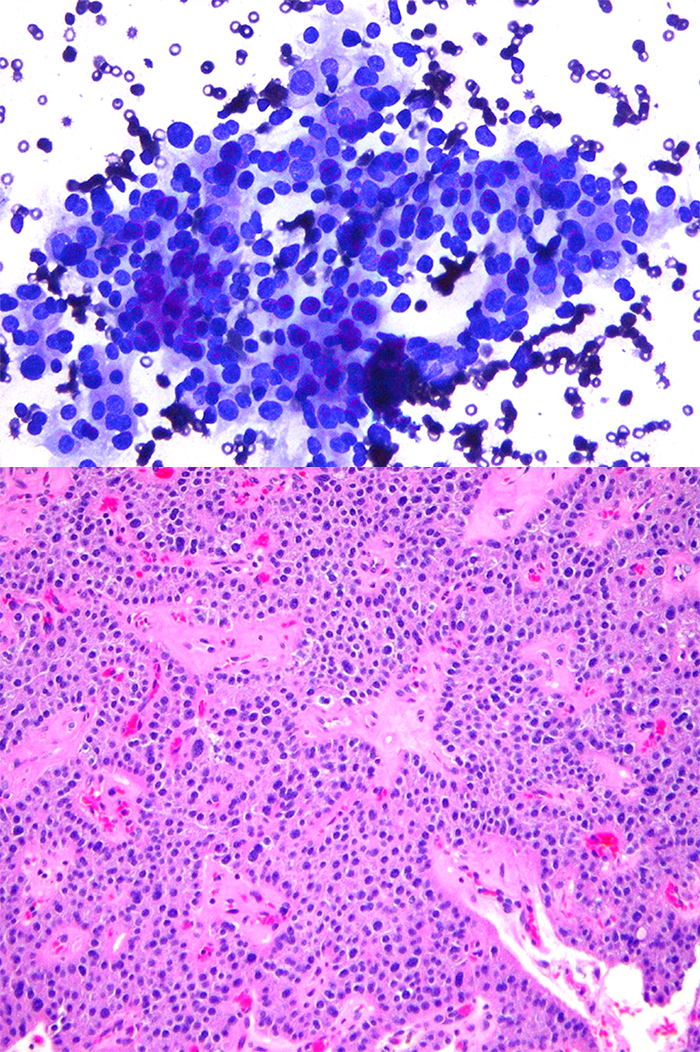
Direct smears from 4 needle passes include occasional clusters of epithelial cells on a background of fresh blood. The cells were uniform and polygonal with microfollicular structure. Cell junctions were generally preserved. Cells had a moderate amount of granular eosinophilic cytoplasm. At high magnification the nuclei were uniform, small and round without chromatin atypia. Small chromocenters were noted, but no macronucleoli were seen. Some groups showed transgressing vessels (Fig. 2-1). There was inadequate material for ancillary immunohistochemical studies to confirm a diagnosis of parathyroid cells. Thyroid mutation panel for ThyroSeq was performed.Diagnosis
Follicular Neoplasm/Suspicious for Follicular Neoplasm. A parathyroid lesion cannot entirely be excluded (Bethesda 2017 Category IV). Thyroid mutation panel is requested.ThyroSeq Molecular Test Result.
Positive with strong expression of Parathyroid gene.
Follow-up
Pre-operative evaluation shows no evidence of metastatic disease related to the thyroid or kidney; curative surgery confirms the diagnosis of parathyroid adenoma (Fig. 2-2). -
A 56-year-old Asian woman presents with a long history of multinodular goiter; sonography confirms multiple solid and cystic nodules. The largest nodule is located in the isthmus and measures 1.5 cm. The patient is referred to radiology for FNA of the dominant nodule.
Cytopathology
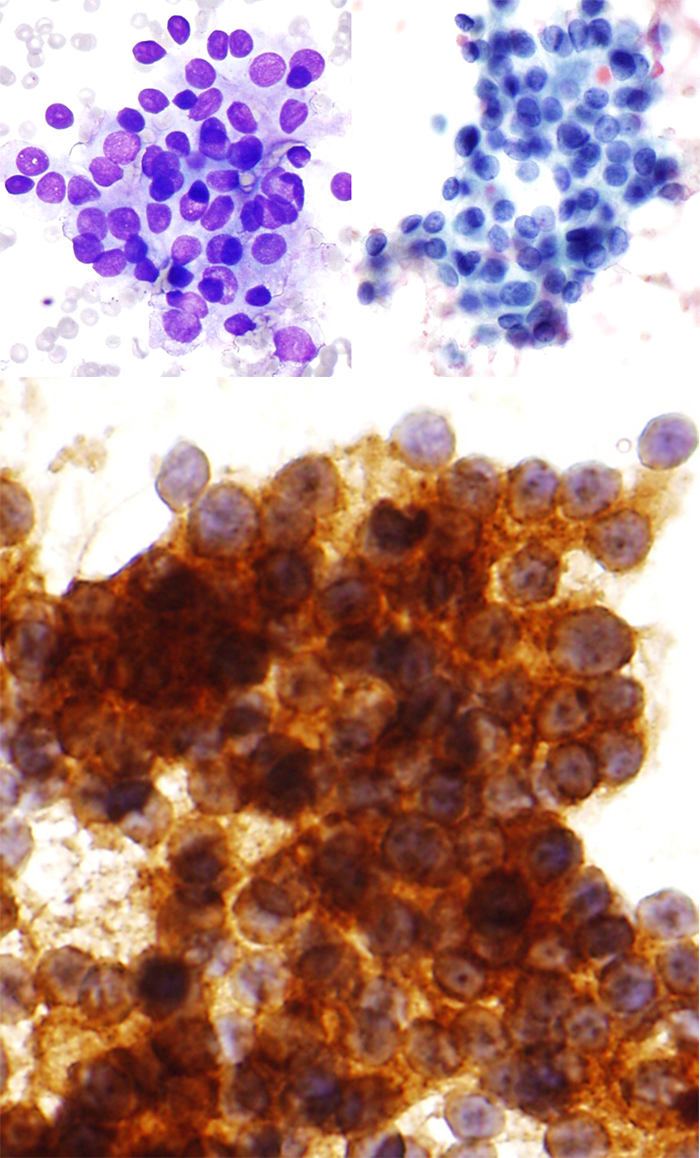
The background was mainly fresh blood with some dense colloid. Monolayer crowded clusters of atypical cells were identified; atypia was characterized by uniform moderate nuclear enlargement with increased N/C ratio, and a variety of nuclear membrane defects. Focal chromatin clearing and intranuclear grooves were present; however, optical clarity and nuclear pseudoinclusions were not seen (Fig. 3-1 TOP). No papillary structure or psammoma body were identified. CK-19 immunostain was strongly positive (Fig. 3-2 MIDDLE).
DiagnosisSuspicious for Malignancy; Suspect Papillary Thyroid Carcinoma, Possibly Follicular Variant (Bethesda 2017 Category V). Thyroid mutation panel is requested.
ThyroSeq Molecular Test Result.
Positive for NRAS mutation.
Follow-up
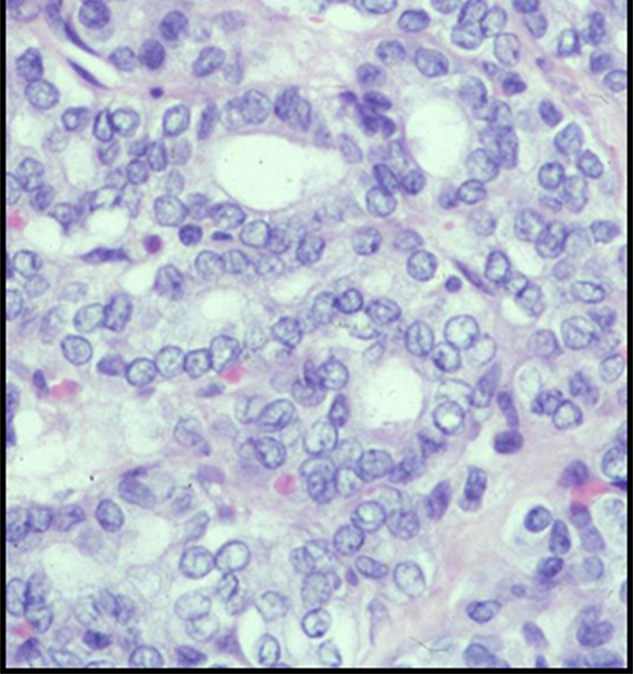
Partial thyroidectomy was performed; surgical pathology diagnosis included several colloid-rich adenomatous nodules, including one with a single 0.3 cm. focus of non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) (Fig. 3-3 BOTTOM). -
A 46-year-old woman underwent drainage of a solitary 1.0 cm. left thyroid cyst. About 0.5 cc. of "airplane glue" material is aspirated and submitted for cytology.
Cytopathology
The background showed abundant dense colloid substance throughout. Scattered small clusters of partly degenerated follicular epithelial cells were present. Several large complex fibro-epithelial tissue particles were identified; at low magnification papillary contours were evident. At high magnification, epithelial cells were palisaded at the periphery of the particles to produce a "community border." However, the nuclei were characterized by ordinary degenerative changes without specific chromatin atypia (Fig. 4-1 BOTTOM). CK-19 immunostain was completely negative .
Diagnosis
Benign follicular nodule, consistent with hyperplastic/adenomatoid nodule (Bethesda 2017 Category II).Follow-up
Clinical/radiologic follow-up is ongoing. At one year after FNA, follow-up remains entirely negative.